Frostbite
Severe frostbite causes ischemic tissue injury that can lead to amputation. Hyperbaric oxygen therapy is an emerging adjunctive treatment that may help salvage threatened tissue when started early.
What is Frostbite?
Frostbite is tissue injury caused by freezing. Living in Vermont, exposure to extreme cold during outdoor work, recreation, or accidental exposure can result in serious cold injury, most commonly affecting fingers, toes, ears, nose, and cheeks.
Beyond the initial freezing of tissue, much of the lasting damage comes from a secondary process: blood vessel injury, microvascular thrombosis, inflammation, and progressive ischemia in the hours and days after rewarming. Deep (3rd-degree) and full-thickness (4th-degree) frostbite can result in tissue death and amputation.
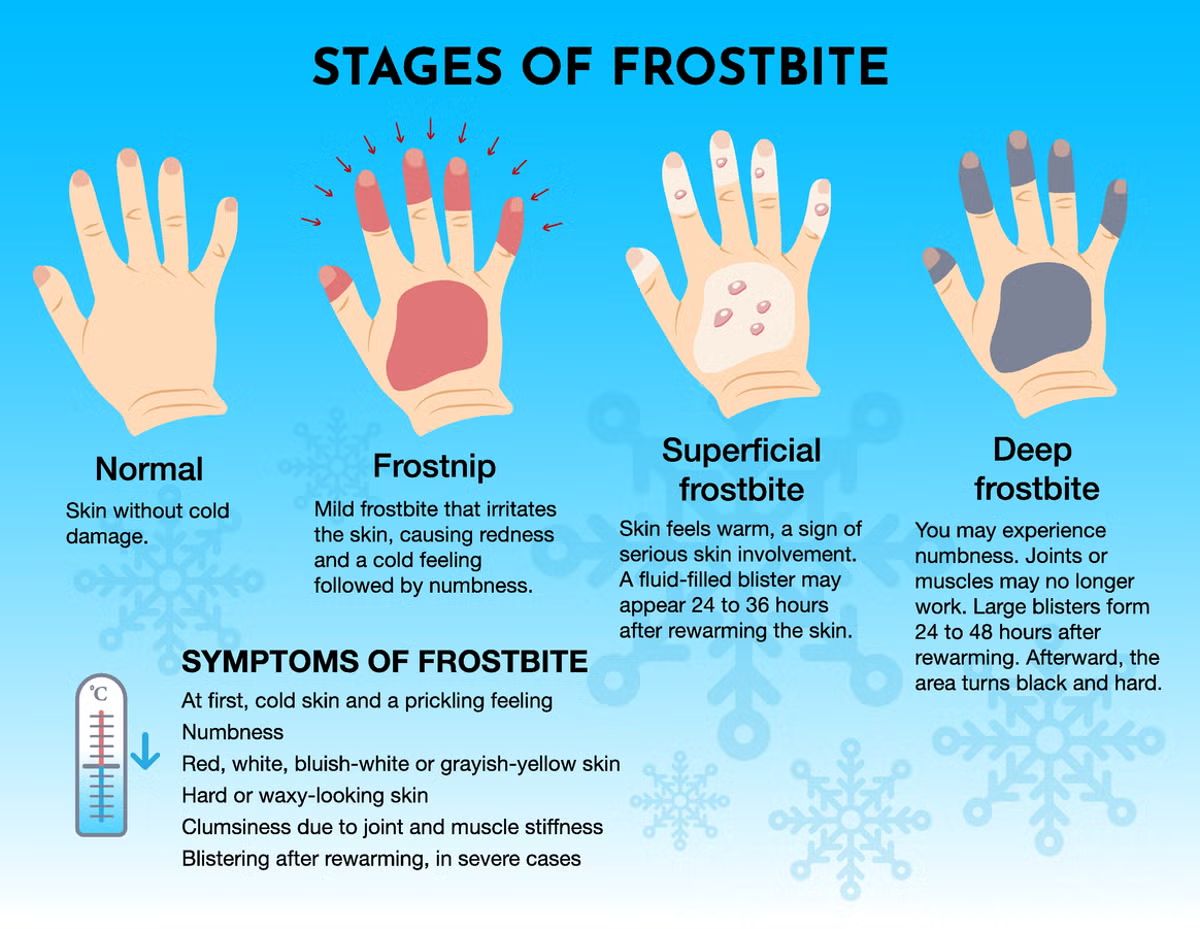
Frostbite is graded in four stages by depth of injury: 1st degree (frostnip) involves only the superficial skin and is reversible; 2nd degree (superficial) produces fluid-filled blisters after rewarming; 3rd degree (deep) causes blood-filled blisters and damage to tissues beneath the skin; and 4th degree (full-thickness) extends through muscle, tendon, and bone. Severity often cannot be fully determined for several days to weeks after the initial injury.
The Four Stages of Frostbite
From frostnip to full-thickness tissue loss — a clinical reference
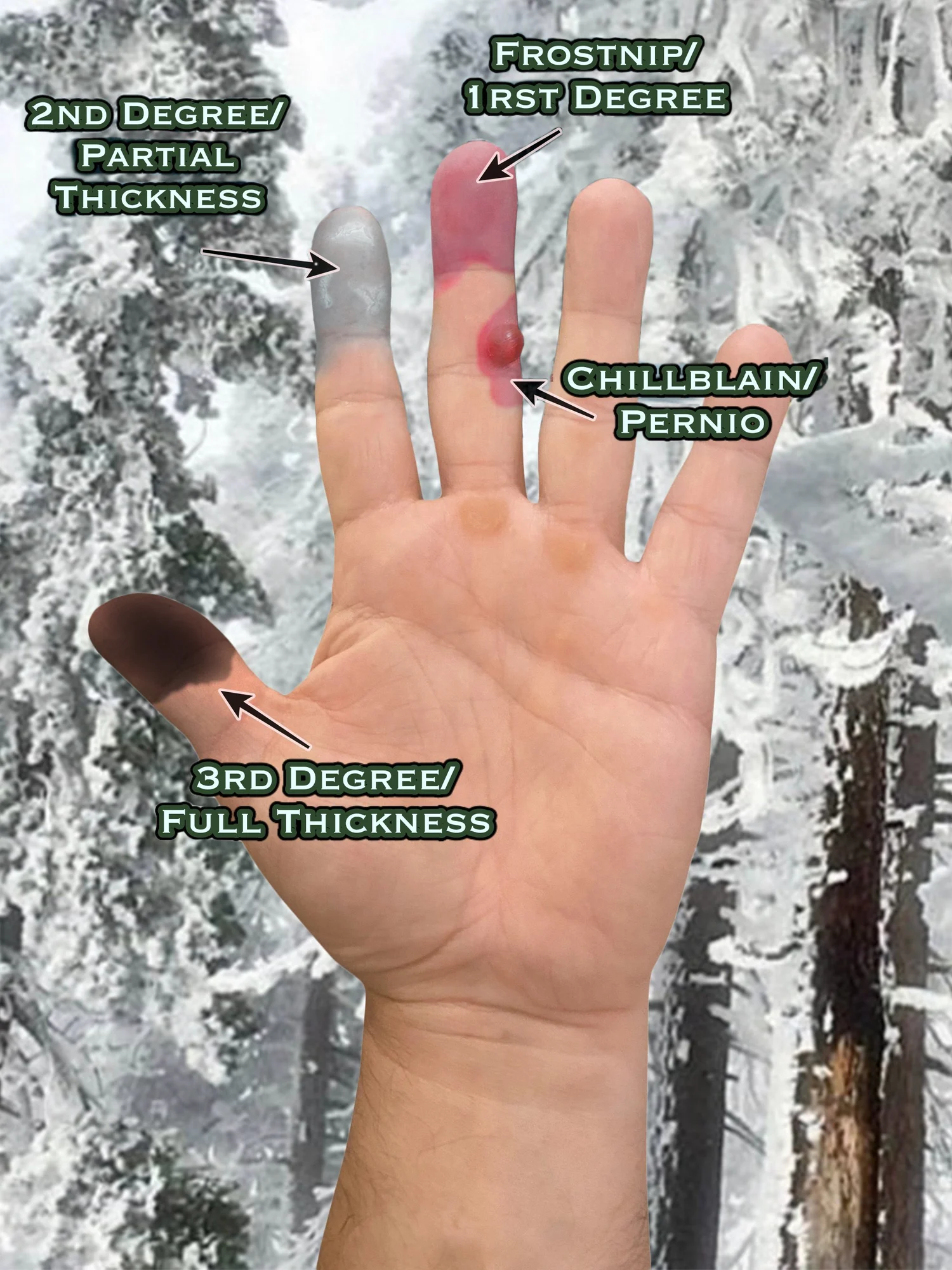
1st Degree
Frostnip
The earliest stage, featuring red, painful, and numb skin with a "pins and needles" sensation. There is no permanent skin damage, but it requires prompt rewarming, after which the skin may peel like a sunburn.
2nd Degree
Superficial Frostbite
The skin becomes firm to the touch but the deep tissues remain soft. Skin may turn pale, white, or blue-gray, and fluid-filled blisters usually form 12 to 36 hours after rewarming.
3rd Degree
Deep Frostbite
Damage extends deeper into the skin and tissue. The skin feels hard and cold, and blood-filled (hemorrhagic) blisters often form, signifying severe damage to the tissues beneath.
4th Degree
Full-Thickness Frostbite
The most severe stage, in which damage extends through the skin, muscle, tendons, and even down to the bone. The tissue dies (necrosis), turns black, and becomes hard, often leading to loss of the affected part.
Why Time Matters: The Four Phases of Cold Injury
Most lasting damage happens after the tissue thaws — which is why early evaluation is critical.
- 1
Cooling & Freezing
Vasoconstriction shunts blood away from the extremities to protect core body temperature. As cold persists, ice crystals form inside and around cells, disrupting membranes and dehydrating tissue. Sensory nerve dysfunction begins around -10°C.
- 2
Rewarming
Ice crystals melt, capillaries become leaky, and fluid extravasation produces blisters and edema 6–24 hours after rewarming. Preventing a second freeze-thaw cycle is critical — repeat freezing dramatically worsens outcomes.
- 3
Progressive Tissue Injury
Inflammation, microvascular thrombosis, and a shift toward vasoconstrictive prostaglandins (thromboxane B2, PGF2α) drive ongoing ischemia. This is the window in which adjunctive therapies — including hyperbaric oxygen — may help limit the final extent of tissue loss.
- 4
Resolution & Demarcation
Outcomes range from complete healing, to healing with sequelae, to clearly necrotic tissue. The line between viable and nonviable tissue often takes 1–3 months to fully declare itself — a principle long summarized as "frostbite in January, amputate in July."
Who Is Most at Risk
Vermont winters create real environmental risk — but host factors matter just as much.
Environmental Factors
- •Risk rises sharply below -25°C ambient temperature
- •Wind chill: skin can freeze in 10 minutes at -18°C with 40 mph winds
- •Prolonged duration of exposure
- •Altitude above 17,000 feet
- •Direct contact with conductive materials — water, ice, or metal
Host Factors
- •Tobacco use — reduces nitric oxide and promotes thrombosis
- •Alcohol intoxication — dulls the shivering response and impairs judgment
- •Prior cold injury — leaves tissue permanently more vulnerable
- •Peripheral vascular disease, diabetes, and Raynaud's phenomenon
- •Inadequate footwear — thermal insulation is the single most important preventive measure
Long-Term Effects After Frostbite
Even after the wound heals, sequelae can persist for years — early, comprehensive care helps minimize them.
Persistent Pain
Roughly half of adults report chronic pain in the affected area; in a meaningful subset, it is severe enough to limit daily activity.
Cold Sensitivity & Vasospasm
Lasting Raynaud-like color changes, hyperhidrosis, and exaggerated cold intolerance are common — often worse on the first cold day of every winter.
Neuropathy
Numbness, tingling, and altered temperature perception reflect injury to small sensory nerves and may persist long after the skin has healed.
Joint & Bone Changes
Frostbite arthropathy can produce subchondral bone loss and joint contractures, particularly at the small joints of the fingers and toes.
Skin & Nail Changes
Thinned skin, persistent discoloration, and dystrophic nail growth can mark previously frozen tissue indefinitely.
Tissue Loss
Deep frostbite may ultimately require amputation of fingers, toes, or larger structures — typically only after the boundary between viable and nonviable tissue has fully declared itself.
Signs and Symptoms by Stage
If you or someone you know is experiencing these symptoms, seek medical attention. Early intervention is critical for many of these conditions.
- 1st degree (frostnip): red, painful, numb skin with a 'pins and needles' sensation; skin may peel after rewarming
- 2nd degree (superficial): firm, pale, white, or blue-gray skin with clear fluid-filled blisters 12–36 hours after rewarming
- 3rd degree (deep): hard, cold skin with blood-filled (hemorrhagic) blisters and damage to deeper tissue
- 4th degree (full-thickness): blackened, mummified tissue extending through muscle, tendon, and bone
- Severe pain, throbbing, or burning during rewarming
- Persistent cold sensitivity, numbness, or pain in healed areas
Comprehensive Frostbite Care
Modern frostbite management is time-sensitive and multidisciplinary. Care typically begins in the emergency department and may continue with wound care, hyperbaric medicine, and surgery.
Rapid Rewarming
Controlled warm-water rewarming of the affected tissue is the cornerstone of initial treatment and should be performed in a medical setting whenever possible.
Wound Care
Specialized dressings, blister management, and serial debridement of clearly nonviable tissue while preserving any tissue that may recover.
Imaging & Perfusion Studies
Bone scans or angiography help assess depth of injury and tissue viability to guide treatment decisions.
Pain Management & Anti-inflammatory Care
Pain control and medications aimed at limiting the secondary inflammatory and clotting cascade that worsens injury.
How Hyperbaric Oxygen Therapy May Help
HBOT is considered an emerging, off-label adjunctive therapy for severe frostbite — it is not currently a UHMS-approved indication, and the supporting evidence consists primarily of case series and case reports rather than large randomized trials. We discuss benefits, limitations, and the state of the evidence with every patient.
By dramatically increasing the oxygen dissolved in plasma, HBOT can deliver oxygen to tissue beyond areas of microvascular injury and clotting. Reported potential benefits include reduced tissue edema, improved viability of marginally injured tissue, and support of new blood vessel formation during recovery.
Outcomes appear most favorable when HBOT is initiated as early as possible after rewarming, ideally within the first 24–48 hours, and combined with standard frostbite care.
Key Benefits of HBOT for Frostbite
Treatment Protocol
Reported protocols vary, but typical adjunctive HBOT for frostbite uses sessions at 2.0–2.5 ATA for 90 minutes, often once or twice daily early in the course, then daily as the wound stabilizes.
The total number of treatments depends on depth of injury and clinical response, commonly ranging from 5 to 20+ sessions. HBOT is always provided alongside standard rewarming, wound care, and surgical management.
Because evidence is still developing, eligibility, expected benefit, and treatment duration are individualized. Earlier referral generally allows for better-informed decisions.
Related Conditions Treated With HBOT
Patients researching Frostbite often explore these closely related indications for hyperbaric oxygen therapy at our Burlington, Vermont center.
Ready to Explore HBOT?
Schedule a consultation with our hyperbaric medicine specialists to discuss whether HBOT may be right for your condition.